|
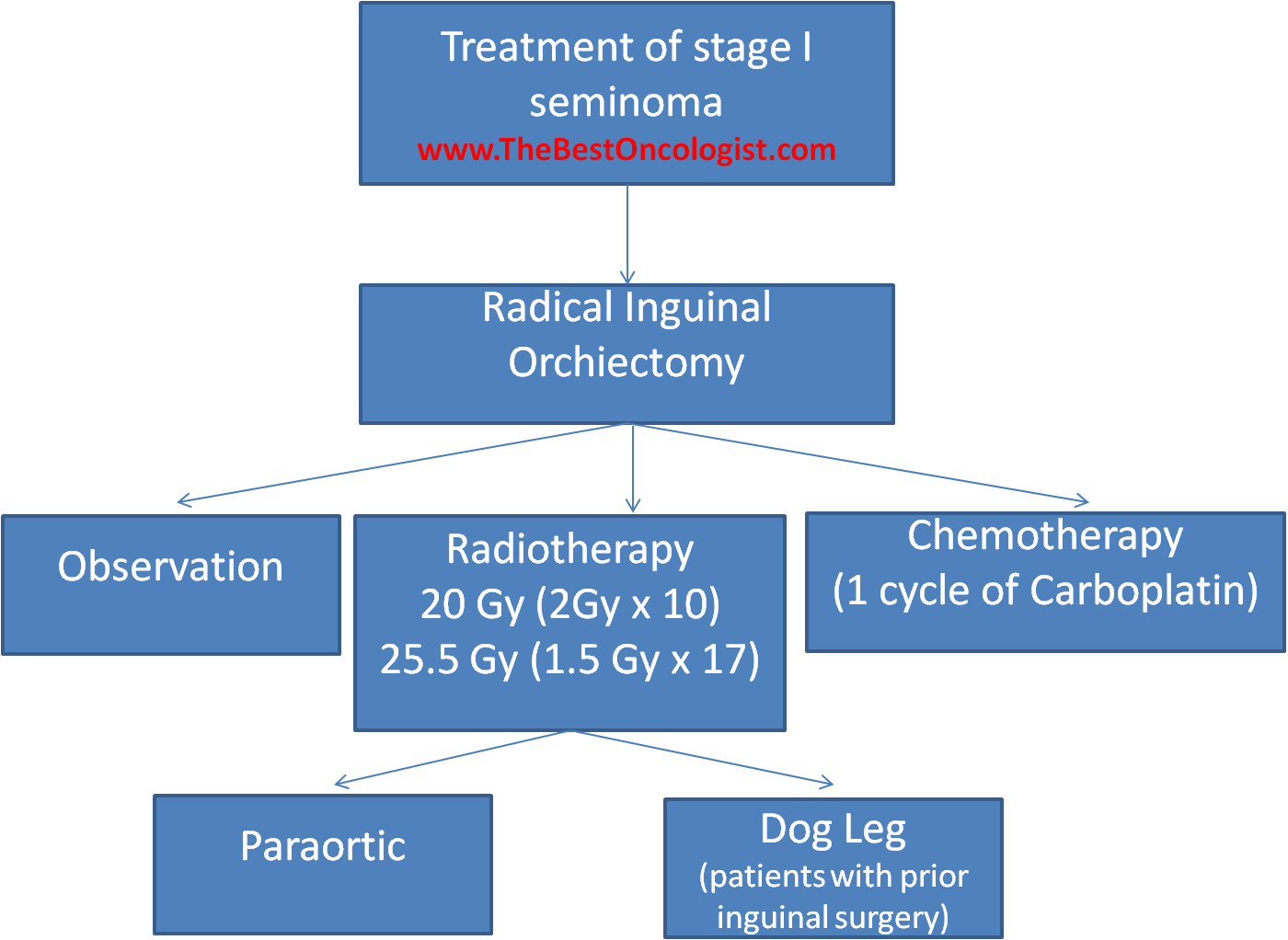
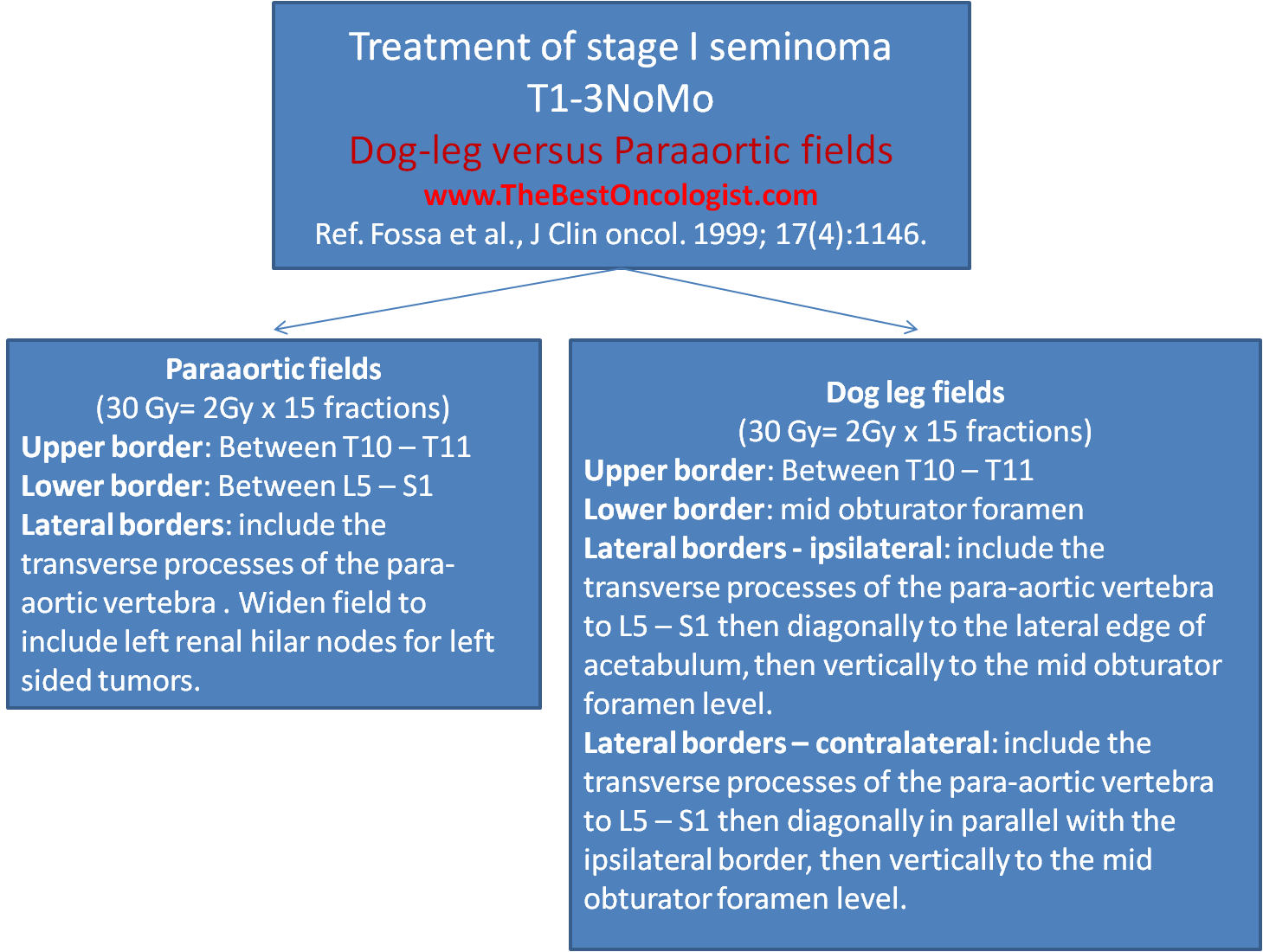
The medical research council testicular
tumor working group randomized patients with
Stage I seminoma and undisturbed lymphatic
drainage to receive paraaortic (PA) or dogleg
(DL) fields. Three years relapse-free survival
was 96% after PA radiotherapy and 96.6%
after DL. Survival at 3 years was 99.3% for
PA and 100% for DL radiotherapy. Nausea,
vomiting, leukopenia was less frequent and
less pronounced in patients in the PA arm.
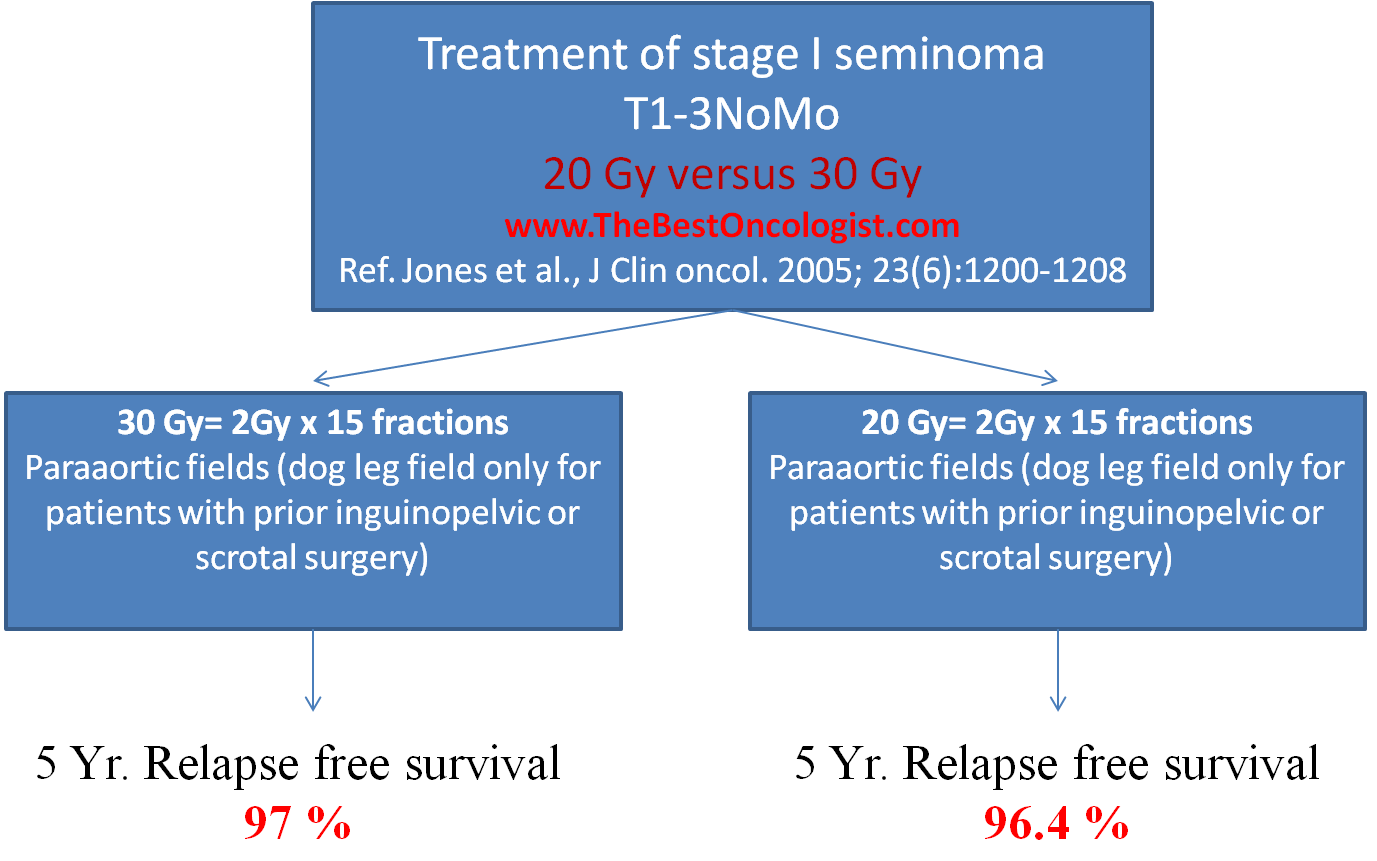
Subsequent trail from the MRC compared low
radiation dose of 20 Gy to the para-aortic
field versus 30 Gy and found that there was
no difference in relpase free survival, but
four weeks after starting
radiotherapy, significantly more patients
receiving 30 Gy reported moderate or severe
lethargy (20% v 5%) and an inability to
carry out their normal work (46% v 28%).
However, by 12 weeks, levels in both groups
were similar.
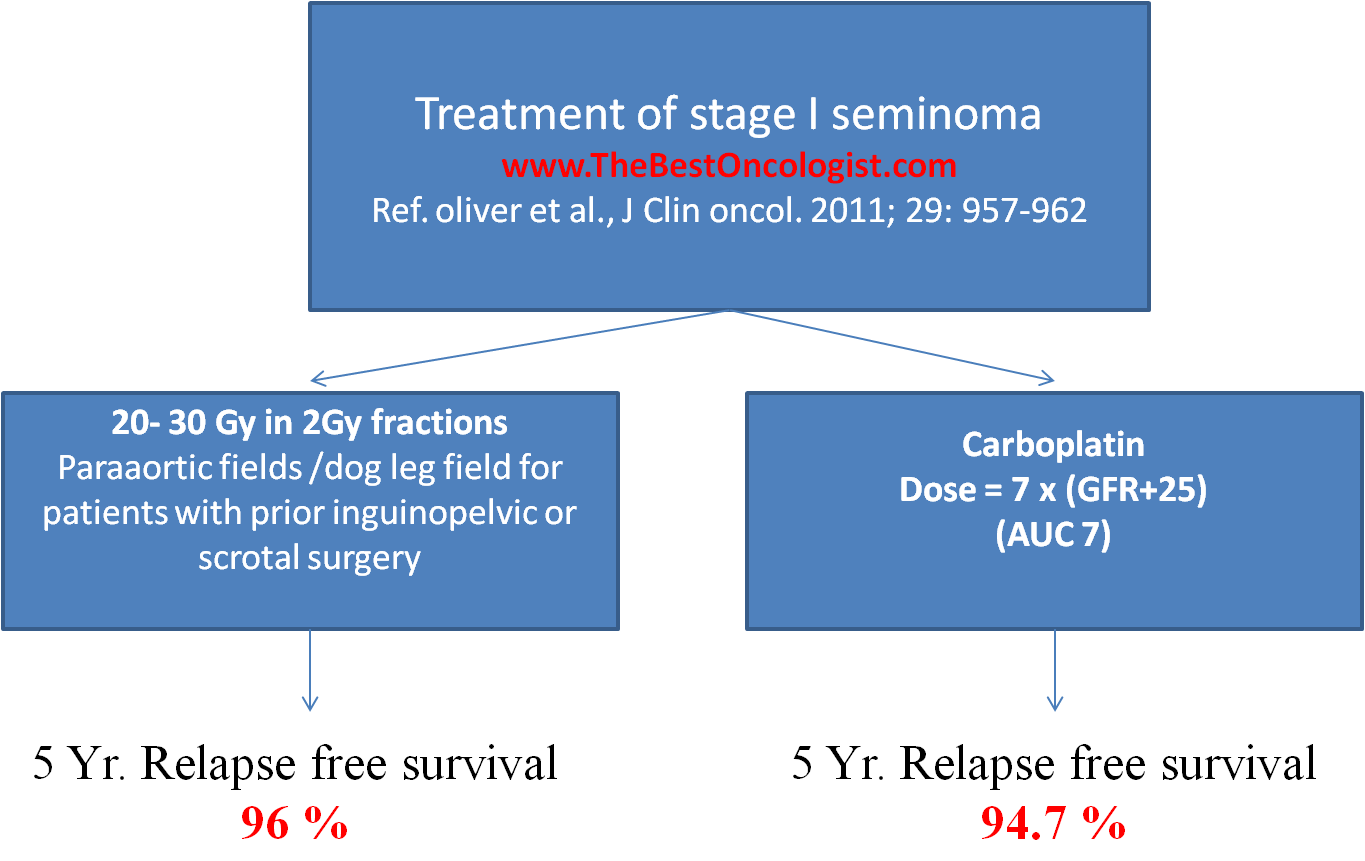
Oliver et al. compared adjuvant treatment of
patients with Stage I seminoma with
radiotherapy (20-30 Gy) versus single agent
carboplatin at a dose of AUC X 7. The
results show noninferiority of single
dose carboplatin versus RT in terms of RFR
and establish a statistically significant
reduction in the risk of second germ cell
tumor produced by this treatment.
Classen modification:
Classen et al described a modified dog leg
field for treatment of seminoma:
Upper border: Between T10 – T11
Lower border: cranial rim of the
ipsilateral acetabulum
Lateral borders - ipsilateral:
include the transverse processes of the para-aortic
vertebra to L5 – S1 then diagonally to the
cranial lateral edge of acetabulum.
Lateral borders – contralateral:
include the transverse processes of the para-aortic
vertebra to L5 – S1 then diagonally in
parallel with the ipsilateral border.
Radiation doses
to stage IIA/ IIB seminoma
Stage IIA seminoma treatment doses: dog
leg field with dose of 2 Gy x 10 fractions
or 1.7 Gy x 15 fractions followed with boost
to involved lymph nodes + 2 cm margin to 30
Gy.
Stage IIB seminoma treatment doses: dog
leg field with dose of 2 Gy x 10 fractions
or 1.7 Gy x 15 fractions followed with boost
to involved lymph nodes + 2 cm margin to 36
Gy.
References:
-
-
-
-
|